100%
4
Rated
Attempts
127
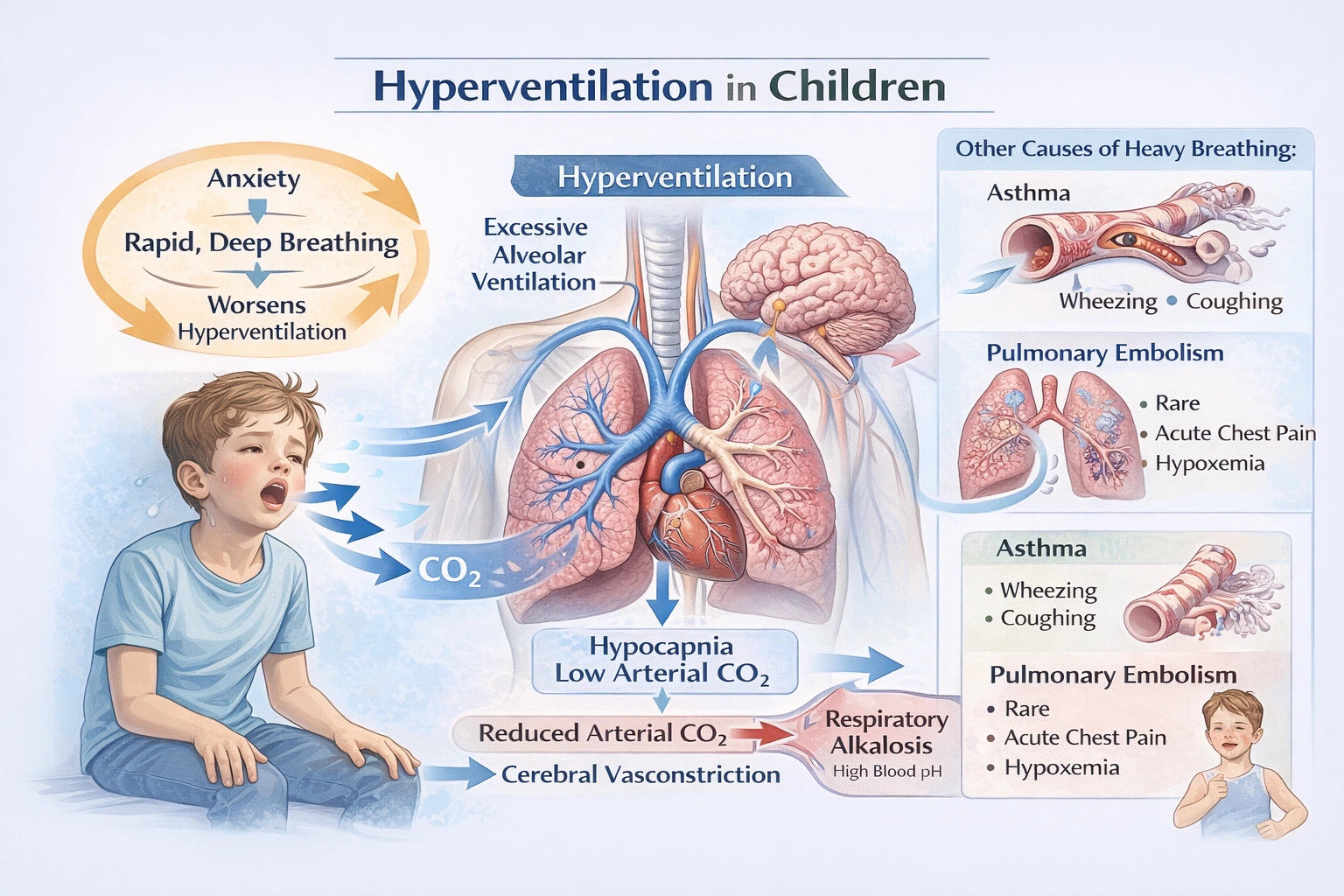
A child complains of heavy breathing even when relaxing. They are an otherwise healthy child with no history of respiratory problems. What might be the issue?
-
A
Asthma
-
B
Blood clot
-
C
Hyperventilation
-
D
Exercising too hard
A
Asthma
B
Blood clot
C
Hyperventilation
D
Exercising too hard
Related Questions
Top Picks
Find the lowest coefficients that will balance the following combustion equation.
What is the purpose of a catalyst?
Most catalysts found in biological systems are which of the following?
Which statement is true about the pH of a solution?
Salts like sodium iodide (NaI) and potassium chloride (KCl) use what type of bond?
Available FREE Test
Sets
Available Test
Sets